Latest update?Be among the first to know by subscribing with my RSS Feed for FREE!Thank you!
 Diagnosis: Emphysema
Diagnosis: Emphysema
Definition:
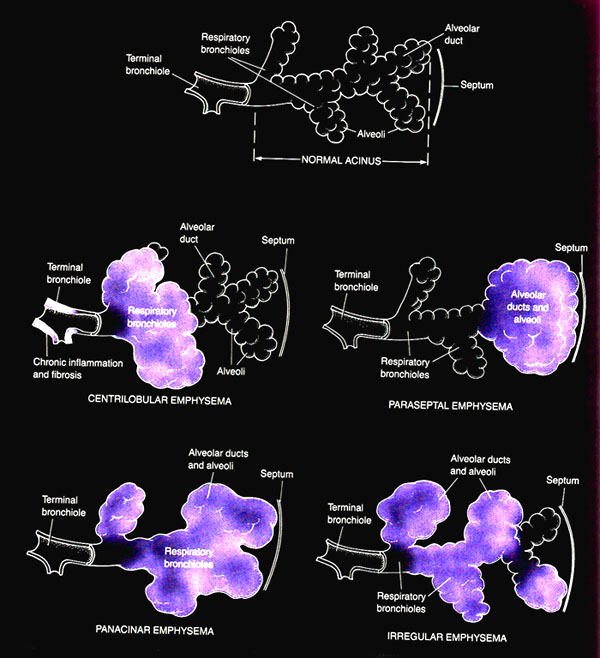
- abnormal permanent enlargement of air spaces distal to the terminal bronchioles, accompanied by the destruction of the walls and without obvious fibrosis
1.Centriacinar(centrilobular)
- begins in the respiratory bronchioles and spreads peripherally
- associated with long-standing cigarette smoking
- predominantly involves the upper half of the lungs
- destroys the entire alveolus uniformly
- generally is observed in patients with homozygous alpha1-antitrypsin (AAT) deficiency
- Among smokers,focal panacinar emphysema at the lung bases may accompany centriacinar emphysema.
- predominant in the lower half of the lungs
- preferentially involves the distal airway structures, alveolar ducts, and alveolar sacs
- process is localized around the septae of the lungs or pleura
- apical bullae may lead to spontaneous pneumothorax
- Giant bullae occasionally cause severe compression of adjacent lung tissue.
Causes:
- Tobacco smoking (mainly)
- Toxic chemicals
- alpha-1-antrypsin deficiency
- air pollution
- genetic
- abnormal airway reactivity
- old age
- Chronic bronchitis
- Bronchitis
- Bronchiectasis
1.neutrophil and macrophage activation and retention in the lung parenchyma
- neutrophils produce serine proteinases
- Macrophages synthesize various metalloproteinases and cysteine proteinases.
- neutrophils and macrophages release elastase
- these enzymes can break down the walls of alveoli which leads to significant modifications of lung architecture.
- AAT is a glycoprotein member of the serine protease inhibitor family that is synthesized in the liver and is secreted into the blood stream
- main function is to neutralize neutrophil elastase in the lung interstitium and to protect the lung parenchyma from elastolytic breakdown
- AAT deficiency predisposes to unopposed elastolysis with clinical sequela of early onset of panacinar emphysema.
- productive cough or acute chest illness-cough usually is worse in the morning and produces small amounts of colorless sputum
- Breathlessness
- Wheezing may occur in some patients, particularly during exertion and exacerbations
- cyanosis
- wheeze
- tachpnoea
- hyperinflation
- cricosternal distance <3cm
- reduce chest expansion
- resonant or hyper-resonant percussion
- quite breath sounds
Test:
Routine:
- FBC=PCV increase
- Chest X-ray=
-Flat hemidiaphragms
-large central pulmonary arteries (due to pulmonary hypertension)
-reduce pulmonary vascular markings
-bullae
-hyperlucency of the lungs
- CT scan
- Pulmonary function test
-FEV1:FVC ration <70%
-TLC-increase
-DLCO-reduce
-RV-increase
- ABG - PaO2 reduce±hypercapnia
- ECG- right atrial and ventricular hypertrophy (cor pulmonale)

